

 Sebo Marketing
Sebo Marketing
 October 18th, 2021
October 18th, 2021





Malocclusion, as an etiological a in dental disease, is among the most controversial subjects in dentistry. Bruxism has been blamed on stress and many other nondental factors. A biomechanical mechanism that serves as a contributing factor to stimulate tooth clenching and grinding is defined and used to identify the 12 common dental symptoms caused by tooth clenching and grinding. A method is proposed, through which the practitioner can link the observable dental signs the biomechanical factors for accurate diagnosis and appropriate treatment, preferably at an early before the damage becomes severe.
Biomechanically induced dental disease affects at least 75% of the adult population. It is likely that more teeth are lost due to biomechanically induced dental disease than to the effects of caries. Nonetheless, caries has been the main focus of the preventive dentistry movement since Arnum and Bass’ theory of bacteria and philosophy of preventive dentistry was popularized by Barkley in the early 1970s. The controversy of occlusal imbalance as a biomechanical etiological agent in dental disease is due primarily to the fact that it is difficult for many practitioners to clinically define and then establish a condylar position in which the condyles can operate in harmony with the biting surfaces of the teeth.’ As a result, apples are compared to oranges and much of the dialogue in the scientific literature cannot withstand the scrutiny of logical analysis. In order to move forward, first it is necessary to define rigidly the terms we use every day and then utilize a method to achieve the biomechanical relationship we have defined easily, predictably, and consistently.
An examination of the literature reveals that most of the controversy about occlusion is not the result of scientifically defined and rigorously applied methods but actually is due to sloppy logic and inconsistently applied biomechanics.
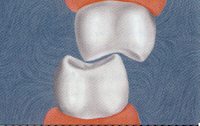
Many people have defined centric relation as the position of the condyles in the glenoid fossa where they are in a stable nonmuscle braced position. Dawson has defined this position as the rearmost, uppermost, midmost (RUM) position of the condyle in the fossa at which the medial pole of the condyle disc assembly is braced against the bony wall of the emenentia. In this position the condyles are supported by the bony structures and muscle activity is balanced and minimized (Fig.1)The teeth, in order to intercuspate fully when swallowing or biting together all the way, can fit together in only one position, just like a key can fit into a lock in only one position.
When the teeth can fit together in a position of maximum intercuspation at the same time the condyles are in the RUM position, they are said to be in a nonconflicted occlusal condylar relationship. If the cusps cannot fit together when the condyles are in the RUM position, the occluding cusps of the teeth act like mechanically inclined planes and actually can force the condyle to deviate from this RUM position to allow for maximum interdigitation. This occlusally determined condylar position requires all of the muscles to contract in an unbalanced and uncoordinated fashion.
It is a testimony to the remarkable adaptability of the temporomandibular joint (TMJ) that it can attempt to accommodate to this conflict. No other joint in the body has the capacity to function in a condition of continuous dislocation.
Realizing that two condyles must coordinate together, one easily can imagine that a very complicated series of muscular accommodation are required for the mandible to move into a position at allows full dental interdigitation Figures 1-3 show only one condyle in two dimensions. In actuality, the two condyles operate three dimensions, which requires geometrically more comlpex accommodations It is rare for a patient to have a condylar relationship that is not in conflict with the occluding surfaces of the teeth. A thorough examination of adult patients reveals at it is equally rare to find one who does not have any signs of biomechanically-induced dental disease that can be proven to result from tooth clenching and grinding.
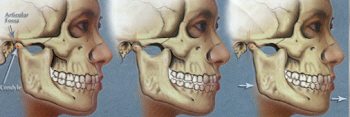
Fig. 1. (Left) Teeth fully intercuspated with he condyles in the RUM position.
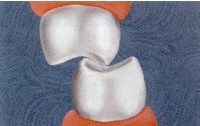
Fig. 2. (Middle) The condyle in the RUM position. Due to a conflict between the teeth and the TMJ, only one tooth can touch its opposing contact.
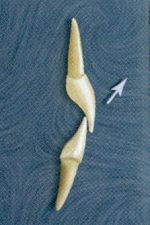
Fig. 3. (Right) The teeth in conflict with the optimal condylar position. Full intercuspation of the teeth results in an eccentric, occlusally determined condylar position.
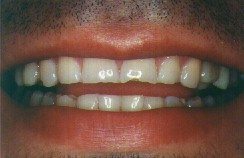
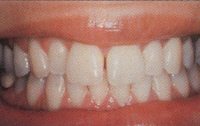
One hundred consecutive patients entering the author’s practice for routine or emergency dental care ere examined clinically and by bitewing and panoramic radiographs and screened by routine medical and dental histories. In addition to bacteria-caused decay and periodontal disease, patients were screened for the 12 biomechanically-induced dental problems that follow. A photograph of each of these dental problems or conditions is provided with a description to illustrate the condition (Fig. 4-15). Although these problems can and usually do occur in combination, they are listed separately.

When you clench or grind your teeth, the nerve inside the tooth may become inflamed. This inflammation of the nerve, or hyperemia, causes tooth pain. The tooth may hurt spontaneously but it is more common for the pain to occur during tooth grinding, normal chewing, and especially when eating or drinking cold foods or beverages. Some people experience so much cold sensitivity in their teeth that they avoid very icy beverages entirely or have to drink through a straw. This inflammation doesn’t cause any structural damage to the tooth and generally is reversible when the clenching or grinding stops. This is similar to what is observed when a dentist places a restoration that has an occlusal interference. The symptoms of sensitivity are relieved when the occlusal interference is reduced.
Clenching or grinding forces can break a tooth. Breakage is especially common in teeth with large fillings because decay and fillings can weaken the tooth and make it more fragile. Usually these teeth can be saved by crowning them but unless the grinding and clenching forces are controlled it is only a matter of time before another tooth will break.

As teeth are ground back and forth in a subconscious attempt to wear down the protruding points, they can become extensively worn. Ironically, though, grinding won’t correct the unevenness that first stimulated it. Tooth grinding follows a back and forth or side to side pattern. Because of the shape of the teeth and the bones of the jaw, every tooth along the path of the grinding experiences some wear.
The teeth that wear the most are often the front teeth, even though the offending uneven points almost always are located on back teeth. The amount of wear varies from slight to extreme depending on the intensity of the grinding. In extreme cases, more than half of the tooth structure can be worn away and the patient may require extensive reconstruction to rebuild the worn tooth structures.
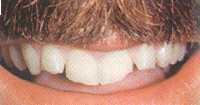
Chipped teeth are worn and fractured teeth. Grinding causes tooth loss from wear. Once teeth are worn down, the tooth structure can become fragile and fracture easily. These chipped regions are seen often on the biting edges of the anterior teeth.

Severe clenching and grinding pressures can cause internal cracks and stress fractures in the teeth. They are not painful and unless they go deep into the tooth they do not compromise the strength of the tooth. They look similar to the maze of crack lines seen in ice cubes that have been hit but not broken. These subsurface stress cracks sometimes can be nearly invisible unless a light beam is angled to reveal them.

When clenching or grinding causes an internal crack deep inside the tooth, the cracked segment can move away from the remaining tooth structure. The crack is usually so small and the movement so slight that it is nearly imperceptible but biting on the tooth at just the right angle can cause severe pain. If the crack does not go all the way down into the nerve canal, the recommended treatment is to put a crown or onlay on the tooth. That holds the broken tooth fragments tightly together so they cannot move and the pain goes away. If the immobilization does not ease the pain, root canal treatment will be necessary. Cracked tooth syndrome usually strikes the back molars where the force is highest.

We generally blame brushing too hard for gingival recession but it can be caused by grinding, too. Pressures on the teeth rock the tooth back and forth in the bone, damaging it below the gingival margin. When the bone is destroyed, the gingiva has no support and recedes as well. This grinding-induced gingival recession is observed most often on the cheek side of the tooth where the bone is normally thin and most easily damaged. Depending on the degree of recession, it may be necessary to perform reconstructive gingiva procedures as well as correcting the bite.

From gingival recession, the exposed root surface may become sensitive to air sweets, or cold. These areas also are prone to decay.

Just as the wind can cause tall buildings to lean, powerful clenching and grinding forces can bend teeth. When this happens, the enamel near the gingival margin can break off, causing notches in the teeth. These notches are smooth and may or may not be sensitive. Abfractures also can occur on the biting surfaces of back teeth, It is important to realize that these holes are not caries; rather, they are symptoms of grinding or clenching.
When an orthodontist moves a tooth, the braces exert forces so small they are measured in ounces. On the other hand, grinding or clenching can create forces of 500 pounds per square inch. Forces of that magnitude can cause considerable undesirable tooth movement. Movement usually is noticed first when spaces develop between the top front teeth or where the lower front teeth begin to overlap.
This problem once was blamed on third molars pushing the other teeth. But the third molar buried in the back of the jaw could never exert enough force to affect a front tooth. When you park your car, it can’t move seven cars in front of you to create extra space. In the same way, third molars can’t move all of your teeth from the back up to the front to shift the front ones. Any time teeth shift, a problem in the bite should be suspected and investigated.

If the bone that holds the teeth in place is damaged, the teeth can become loose. Usually bone damage is associated with plaque and periodontal disease. However, it is evident that prolonged grinding or clenching also can damage the bone.
A tooth that is held by healthy strong bone is never perceptibly loose. At the first sign of loose teeth, the dentist must carefully examine the gums for symptoms of infection and the bite for signs of unevenness, occlusal trauma, and fremitus. Often all are present.

Except for decay or accidents, tooth loss usually is caused by bone loss or tooth breakage beyond the point of repair. Both of these conditions, loosening and tooth breakage, often are caused by tooth clenching and grinding.
The same excessive biting force that can cause pain in one tooth or break another tooth can loosen another tooth painlessly. The cause is the same. The resulting damage depends on the resistive capacity of the individual.
Of the 100 patients, all were found to have one or more of the 12 listed biomechanically-induced dental signs and symptoms.
The table shows the 12 dental signs and symptoms and the number of times that each one was found. If a patient had one or more abfractures, for example, they were counted as one even if there were six teeth with abfractures, so the maximum reportable number of any of the signs was 100.
In order to substantiate the use and effect between the dental sign and biomechancial forces of tooth clenching and grinding, the following requirements were established. In every situation in which trauma was thought to be a causative agent, such as gingival recession, it had to be clear that the patient in fact was grinding his or her teeth based on supporting physical evidence such as ear, hypermobility, and objective evidence such as obvious heavy markings using occlusal indicator ribbon on the affected tooth. The twelfth sign, missing teeth, is highly subjective and is included as a consequence even though the criteria actually are unreliable and impossible to count.
It was observed that most reported biomechanically induced dental signs occurred in multiple situations. For example, most people who exhibited abfracture lesions also had gingival recession, bone loss, and often tooth sensitivity in the same area.
| Dental Condition | % of Patients Exhibiting Condition |
|---|---|
| Abfractures | 56 |
| Broken teeth | 30 |
| Chipped teeth | 73 |
| Cracked teeth | 20 |
| Gum recession | 60 |
| Internal Cracks | 53 |
| Loose teeth | 16 |
| Lost teeth | 6 |
| Root exposure | 56 |
| Sensitive teeth | 53 |
| Shifting teeth | 16 |
| Worn teeth | 96 |
The field of medicine and dentistry has come to associate tooth clenching and grinding with the controversial field of head, neck, and facial pain while ignoring the obvious effect of biomechanically induced dental disease. Despite the fact that structural engineers have studied and quantified the effect of stress in mechanical systems and their response, many dentists seem to believe that the teeth and dental structure somehow are immune to the laws of physics.
There are three basic forces that physical objects can be subjected to, based on the direction of the application of the load. They are compression, tension, and shear Compression force occurs when force is applied in the long axis of the system, such as when a carpenter hits a nail straight into a piece of wood. Tensile force occurs when the direction of the force is between 180 degrees and 90 degrees of the long axis. Shear force occurs when force is directed perpendicular to the long axis. Experience tells you that no matter how hard a nail is struck and regardless of the weight of the hammer, a nail that is hit with the force directed in the long axis of the nail will never bend.
On the other hand, when the nail is struck off axis, the nail will be bent with even minimal force. That is because any system can withstand compression forces 60 times greater than tensile and shear forces without deformation. The most destructive application of force is shear force where the force is directed perpendicular to the long axis of the system. Every mechanical system is designed to put as much of the load as possible into compression. When that is not possible, the strength of the design must be enhanced to accept and resist the significantly greater forces that are delivered in tensile or shear.
Consider the dental system from an engineering point of view. In a typical dentition with normal overbite and overjet of the anterior teeth, the posterior teeth, in vertical closure, have the potential to be subjected to nearly vertical compressive loading. Even though the mandible closes on an arc of rotation, if the biting surfaces contact in the line of the long axis of the teeth, the potential force is nearly vertical in the molars and premolars just like the force of the hammer is on the nail (Fig. 16).

If the teeth hit off axis, the force becomes a combination of tension and shear with some compression (Fig. 17).
In lateral or protrusive excursions, any forces on the posterior teeth must be primarily tension and shear (Fig. 18).
In the case of the upper anterior teeth, due to the overbite and overjet, the force they are subjected to in vertical closure is always a combination of tension and shear. The same is true in lateral excursions or protrusive excursions (Fig. 19).

In the case of the mandibular anterior teeth, a close examination will reveal that a great percentage of the force directed at the lower anterior teeth actually is directed in compressive; during vertical closure and even during excursions much of the force is in compression (Fig. 20).
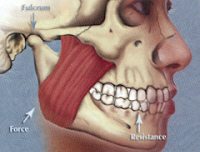
The engineering design of the maxilla and mandible is a classical class II lever system in which the TMJ is the fulcrum, the muscles are the force, and the teeth or bolus of food acts as the resistance (Fig. 21).
In any lever system, the resultant force is always proportional to the square of the distance from the fulcrum. Therefore, it would be expected that the force in the molar area would be considerably greater than in the incisors.
Had the human chewing system been designed by structural engineers, they would have had to evaluate the strength of the teeth and bones of the jaws as well as the potential forces that the system would encounter. The two forces to be most concerned about would have been that required for chewing and tearing food and the potential parafunctional forces of tooth clenching and grinding. From a chewing point of view, ripping and tearing foods such as carrots and hard breads and tearing bites out of meats are more difficult than grinding down foods once they have been torn off and wetted and softened by saliva.
The design specifications for incisors show one root per tooth. They generally are conical and the shortest roots in the mouth, with the least surface area. Compare that to the engineering specifications for molars, which have two to three roots per tooth. Roots are elliptical in design and the total surface area for molar roots is typically at least four times that of incisor roots.
Obviously our hypothetical engineers anticipated much more force in the molar area than in the incisor area. There were two reasons for this. First, despite the potential for optimal biomechancial loading of the posterior teeth, they recognized that it was unlikely that the posterior teeth would erupt into an ideal position where vertical loading would be consistent. Instead, nonvertical occlusal contacts would subject the molars to far greater tension and shear forces. This would be magnified greatly because the molars are close to the TMJ.
Second, they recognized the potentially severe destructive forces from parafunctional tooth clenching and grinding. As a result of off-axis loading, proximity to the fulcrum, and parafunctional activities, the molars required strengthening the specifications of the molar roots.
Consider the patients in your practice who are nearly completely edentulous. Which teeth typically are the last to be lost? Think of your own patients and see if you don’t agree that the mandibular incisors, the ones with the smallest roots, often are the last to be lost, even if they have significant bone loss and some mobility.
One reason for this is that the molars are so much closer to the fulcrum that they are subject to much more force than the incisors. The molars can generate forces up to 500 pounds per square inch, while the incisors can generate barely 150 pounds per square inch. In the natural state of the molars, much of the occlusal force is in tension and shear despite the potential for transforming that force into compressive. This explains why there is such a high prevalence of biomechanically-induced dental disease in the general population.
The clinical dentist has the opportunity to intercede and reengineer the system to reduce the potentially destructive biomechanical loads on the teeth and the bones of the jaw through occlusal equilibration and selective reshaping of the biting surfaces of the teeth. The decision of when to intercede has to be based on clinical evaluation of the presence of the 12 dental signs and symptoms of biomechanical dental disease. A patient displaying the damage shown in Fig. 4-15 needs treatment. Patients without significant signs or symptoms of biomechancial dental disease should be made aware of their occlusal disharmony and told that since there does not appear to be any damage, no treatment is indicated at this point.
Step 1 – Assist the condyle to assume the RUM position and perform selective reshaping of the teeth (in general, primarily the posterior teeth) to eliminate any deflective contacts until the posterior teeth can contact equally and simultaneously on both sides without pulling the condyles out of their centered RUM position. Make sure that all contacts are on flat surfaces and cusp tips so that forces are directed primarily in the long axis of the tooth roots to create primarily compressive loads on the posterior teeth.
Step 2 – Slightly relieve anterior teeth in vertical closure so that the off-axis loads do not cause the teeth to move with hard vertical closure. This can be tested by feeling for vibration with your finger or looking for movement of the maxillary anterior teeth with hard vertical closure. This reduces the tension and shear forces on the anterior teeth.
Step 3 – Reshape the posterior tooth inclines so that there is no contact in lateral or protrusive excursions. Allow the canines to bear the load during lateral excursions and the incisors to share the load during protrusive. If the canines are missing, if their bone support is compromised, or if they are out of ideal position, it may be necessary for the premolars to share the load during lateral excursions. This takes the most potentially destructive tension and shear forces off the molars and moves them as far from the fulcrum as possible.
Step 4 – Let the patient tap, clench, and grind his or her teeth in all directions and relieve any posterior tooth inclined plane contacts and reduce any anterior teeth contacts that move the teeth.
Step 1, creating a condylar directed occlusal pattern rather than letting the teeth establish the condylar position, is critical in achieving a harmonious relationship between the biting surfaces of the teeth, the TMJ, and the neuromuscular system. Unfortunately, the average patient has been forced to accommodate to a tooth-directed condylar position for so long that the muscles become cramped and resist the condyles seating to the RUM position.
There are several methods that can be used by the clinician to assist the patient. The first and most difficult for most clinicians is to manipulate the mandible into the RUM position. Stuart called this “romancing the condyle,” while Dawson has described a two-handed technique Both of these and other similar methods, while excellent and highly predictable for a very experienced clinician, are very technique sensitive and are prone to cause errors by the less experienced clinician. These manipulative errors may lead many clinicians to the incorrect conclusion that condylar directed occlusion is not correct, effective, or necessary when the real problem is that this position was not achieved in the first place.
To assist the clinician in positioning the mandible to achieve the RUM position, there are many methods of discluding the posterior teeth so that the condyle is freed to move into the RUM position. This method has been advocated in dentistry for many years. just to name a few of the options, there is the anterior leaf gauge and the central bearing point on custom designed clutches as well as laboratory fabricated splints and custom fabricated splints. All of these, when used correctly, can be very successful in allowing the condyles to achieve the RUM position.
The problem with these systems is that they require a learning curve, they can be cumbersome to use, many cannot be used unassisted by the patient prior to the visit, and some cannot be put on and removed from the teeth easily during equilibration procedures. The biggest barrier to effective treatment and greatest source of controversy in this area is the difficulty of positioning the condyles in centric relation position. For this reason, more effective methods must be developed that are simple to use and easy to learn.
The human stomatognathic system functions like any mechanical system. If the biomechanical forces it is subjected to can be controlled, damage to the system can be minimized. If the biomechanical forces it is exposed to exceed its resistive capacity, damage will occur in the weakest element. Because the damage may show up as broken, sensitive, worn, or abfractured teeth; gum recession; bone loss; mobile, migrating, or ultimately lost teeth; or head, neck, and facial pain, the dentist must be aware of the many potential manifestations of biomechanically-induced dental disease. Further, it is the responsibility of the dentist to discover these signs and symptoms as early as possible and then take action to control these biomechanical forces to minimize their potential consequences.

 M Usman
June 9th, 2026
M Usman
June 9th, 2026
Is Botox Good for Head, Neck, or Facial Pain? Chronic head, neck, and facial pain—especially migraines—affects millions of people. One…
 M Usman
June 9th, 2025
M Usman
June 9th, 2025
When Headaches or Migraines Just Won’t Go Away… Headache? Take a pill.Stress headache? Reduce stress… and take a pill.Tension headache?…
 M Usman
May 19th, 2025
M Usman
May 19th, 2025
Are you tired of dealing with frequent headaches that seem to interrupt your life? Have you sought help from various…